Advances in Rigid Fixation in Maxillofacial Surgery
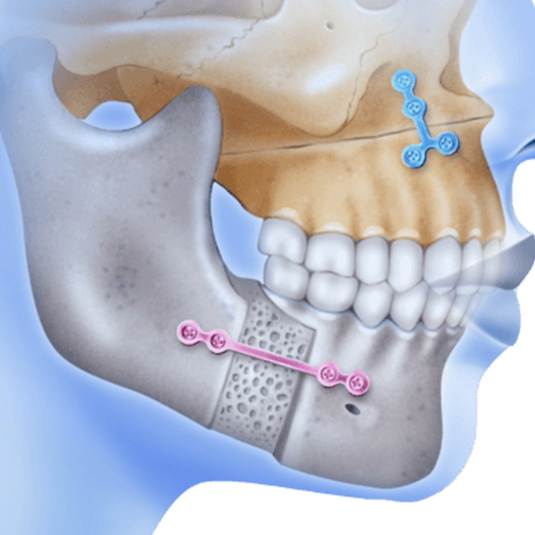
Plate osteosynthesis has become a popular method in securing rigid fixation at fracture and osteotomy sites in maxillofacial surgery. Plating provides an effective means of stabilizing bone, thereby providing an optimal environment for healing to occur. Because plate fixation does provide rigid osteosynthesis, in most cases intermaxillary fixation is not required. The plating systems currently available can be classified into compression and noncompression types.
Compression plates, by virtue of their biomechanical design, provide active compression at the fracture site, thereby promoting primary bone healing. The holes in compression plates are oval and the screws are placed in an eccentric fashion in these holes. As the screws are tightened into the bone, the head of the screw contacts the side of the hole and then, as the screw further countersinks itself into the plate, it forces the bone ends together in an active compression fashion. These screws are typically bicortical in the mandible and therefore must be applied below the level of the mandibular canal. They also may be used in the middle part of the face, with active compression being ideal at the frontozygomatic suture in cases of LeFort III or zygoma fracture.
When plating LeFort I fractures, care must be taken not to utilize compression in the middle part of the face, as it is not necessary and, more importantly, may distract the maxilla, causing a malocclusion. Plates may be placed through either the intraoral or extraoral route depending on the site and preference of the surgeon.
The noncompression or miniplates act in the mandible to neutralize tension or spreading forces along the alveolar border rather than providing active compression at the fracture site. Instead of being placed along the inferior border with bicortical screws, they are placed along predetermined lines of osteosynthesis, which, in the body of the mandible, corresponds to an area between the mandibular canal and the apices of the teeth. These screws are placed in a monocortical fashion, thereby avoiding tooth root injury unless inadvertent deep drilling is done. They are also used in midface osteosynthesis and provide a rigid form of fixation here like that provided by the compression plates. These plates are smaller and more easily bent than compression plates and are designed to be placed primarily through the intraoral route both for mandibular and maxillary osteosynthesis.
The variety of plating systems available today are manufactured from surgical stainless steel, Vitallium, and titanium. Special care must be taken when using these new plating systems, however. Components from one system must not be mixed with components of a dissimilar metal from another system as localized electrolytic reactions can occur, with resultant cytotoxic reactions in the adjacent tissues. Thus, Vitallium screws should not be mixed with titanium plates or titanium screws with stainless steel plates. Plate osteosynthesis has revolutionized the treatment of patients with facial fractures. It has eliminated the need for intermaxillary fixation while providing rigid osteosynthesis. The plates have proved to be yet another important tool in the armamentarium of the facial plastic surgeon